Monthly Archives: February 2018
Cesarian Section Birth

Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum.
Painless Vaginal Birth

Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum.
Natural Childbirth

Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum.
Hysteroscopy


A hysteroscopy is a minimally invasive surgical procedure for viewing the cavity of the uterus by inserting a visualizing scope through the vagina and into the cervical opening. Hysteroscopy allows visualization of the inside of the uterus, including the openings to the Fallopian tubes, as well as direct examination of the cervix, cervical canal, and vagina. It is usually done under anesthesia in an operative set-up.
Diagnostic Hysteroscopy with Fractional D&C – this involves inserting the hysteroscope camera to view the inside of the uterus for the purpose of performing a biopsy on the lining of the uterus . This is usually done in cases of abnormal uterine bleeding or when there is a suspected mass in the uterus for biopsy.
Hysteroscopy, Polypectomy – this involves inserting the hysteroscope inside the uterus to visualize the inside cavity to locate the polyp so it may be removed by either scraping or using a hot wire.
Operative Hysteroscopy – this involves the use of an operative scope and a fluid distention media in performing the following:
- Hysteroscopic Polypectomy – use of an operative scope to resect a polyp
- Hysteroscopic Myomectomy – using an operative scope to resect myomas located inside the cavity of the uterus , called submucous myomas
- Hysteroscopic Resection of Uterine Septum – there are women with developmental abnormalities in their uterus where there may remain a septum inside the uterus , causing infertility or recurrent pregnancy loss. This septum may be resected hysteroscopically to unify the cavity of the uterus.
- Hysteroscopic Resection of Uterine Adhesions – Some women may develop intrauterine adhesions (IUA), synechia, or Asherman syndrome from obstetrical or nonobstetrical instrumentation of the uterus or infection of the urogenital tract leading to Abnormal Uterine Bleeding, Infertility, or Recurrent Pregnancy Loss. These adhesions may be removed with an Operative scope.
- Hysteroscopic Removal of Foreign Body – some women may have a retained or fragmented intrauterine device which may be removed hysteroscopically.






Open Surgery

Indications for using laparotomy over minimally invasive surgery are not hard and fast but largely depend on the experience and expertise of the surgeon, availabitlity of enabling tools or not:
- Morbidly obese patient who cannot tolerate the position of laparoscopy or robotic surgery which requires being in the “head down” or Trendelenburg position to make the bowels move out of the operative field.
- Tumor is so big that it will take hours to morcellate the specimen from the abdomen
- Massive adhesions
- Unstable patient conditions where a pneumoperitoneum (instilling carbon dioxide gas into the patient’s abdomen) would further jeopardize the patient’s condition.
- Advanced ovarian
- Lack of experienced surgeon & surgical team
- Lack of a safely functioning lap tower or robot with working instruments
Click image thumbnails to enlarge.








Laparoscopic Surgery

LAPAROSCOPIC SURGERY – refers to a minimally invasive surgery, also known as keyhole or band-aid surgery because the surgery is performed through tiny incisions in the abdomen through which laparoscopic instruments are inserted to accomplish the surgery. A camera, or laparoscope is inserted through the umbilicus and 2-3 other instruments ranging from 0.5-0.8cm are inserted in the abdomen at strategic locations to accomplish diagnostic procedures, management of ectopic pregnancies, removal of ovaries (laparoscopic oophorectomy or just ovarian cysts (laparoscopic oophorocystectomy), myomas (laparoscopic myomectomy) or the entire uterus (laparoscopic hysterectomy), cancer surgery. It has the advantage of minimizing downtime, rapid recovery back to activities of daily living, less chances for post op complications like pain, bleeding and infection and minimal scarring.





Robotic Surgery


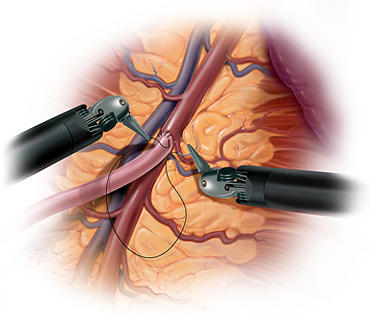
ROBOTIC SURGERY – or robot-assisted surgery is a minimally invasive surgery whereby the surgeon utilizes robotic systems & platforms to allow them to perform complex procedures with more precision, accuracy and control than conventional open surgery or laparoscopic surgery. The surgical robots were designed to enhance the capabilities of open surgery such as the large incisions increasing the chances for post-op pain, wound infection & bleeding, while overcoming the limitations of laparoscopic surgery such as reverse orientation, surgeon fatigue, straight instruments with absence of rotational movements. The Da Vinci Robot was FDA approved for gynecologic surgery in 2005. Robotic surgery can be performed as an outpatient procedure or an overnight procedure, if uncomplicated. Like laparoscopic surgery, it is also a minimally invasive surgery that utilizes tiny incisions or band-aid incisions (since they are small enough to be covered with a Band-Aid). However, it is a more enabling tool, since the instruments have jointed wrist that allow it to have 7 degrees of freedom, more than the human hand and therefore seamlessly and effectively translate the surgeon’s hand movements into the more precise movements of the instrument tips. It eliminates the fulcrum effect leading to reverse orientation inherent to laparoscopic surgery. In contrast to the reverse orientation when doing laparoscopic surgery, the movements in robotic surgery are all intuitive and because the instruments rotate, it is a much easier tool for especially for suturing the defects left when removing a myoma from the uterine wall, or when suturing the vaginal stump to close it after hysterectomy.
In performing laparoscopy, usually the distance of the tissue structure from the port site on the abdomen causes amplification of motion at the instrument tip. This means that a surgeon’s tiny movement with the instruments outside the body causes a relatively large motion on the inside as seen by the camera on the monitor. This can make targeting tissues difficult and frustrating and requires a learning curve to overcome. With the daVinci Surgical Robot, motions are filtered and de-amplified up to a scale of 5 to 1. In other words, the surgeon would have to move the manipulators up to 5 inches in order to cause movement of only an inch on the inside of the body. This is even adjustable to a 3:1 ratio, meaning for every three inches of movement of the surgeon, the machine scales this down to 1 inch of movement of the instruments. This eliminates natural hand tremor entirely, allows the surgeon to target tissues with much greater ease, and gives the surgeon a certain accuracy and refinement that surpasses human capabilities for both the open and standard laparoscopic paradigms.

Dra. Rebecca Singson performing a robot assisted surgery.
Ergonomics is another realm of superiority for the Da Vinci robot. With traditional laparoscopic surgery, the surgeon is standing on the operating table and awkwardly struggling to move the straight instruments manually while keeping the head fixed on the monitor to visualize the movements inside the abdomen. With the Da Vinci robot, the surgeon ergonomically sits on the surgeon’s console, which memorizes the settings for every surgeon. The head is positioned with minimal strain to the neck while looking into the 3-dimensional vision system (laparoscopy only has a 2-diminsional vision system since it has only one camera whereas the robotic camera has 2 cameras: one for the left and another for the right eye). The arms are positioned to the perfect height preferred by the surgeon and the foot pedals are also adjusted to the preference of the surgeon. The vision system allows depth perception because of the 3-dimensional design and the ergonomic set up of performing surgery while seated on the surgeon’s console all translates to eliminating fatigue, especially for complicated surgeries that go on for several hours.




Open Surgery

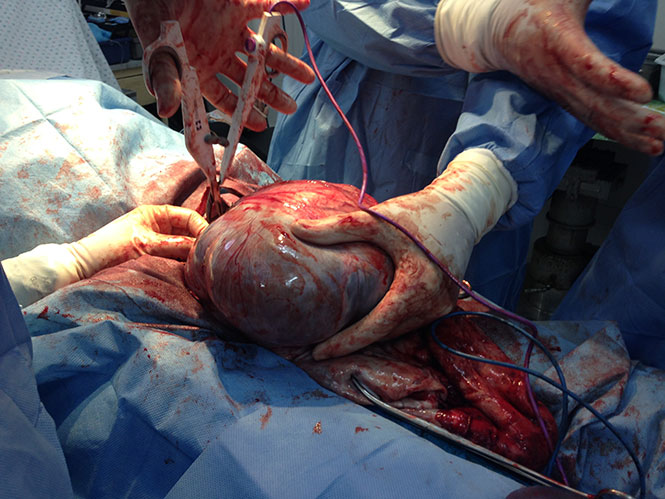
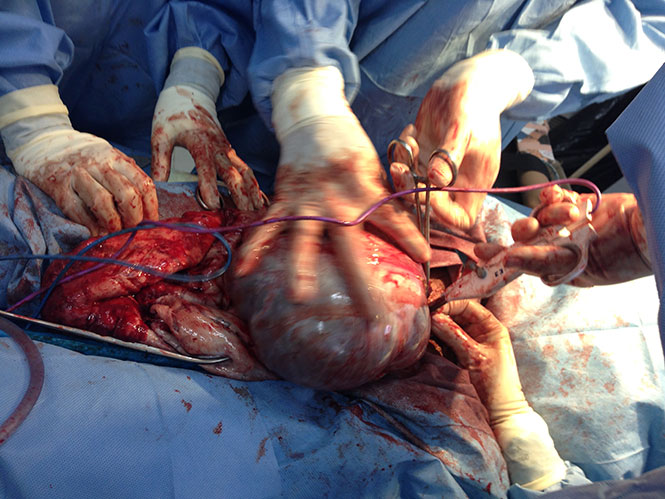
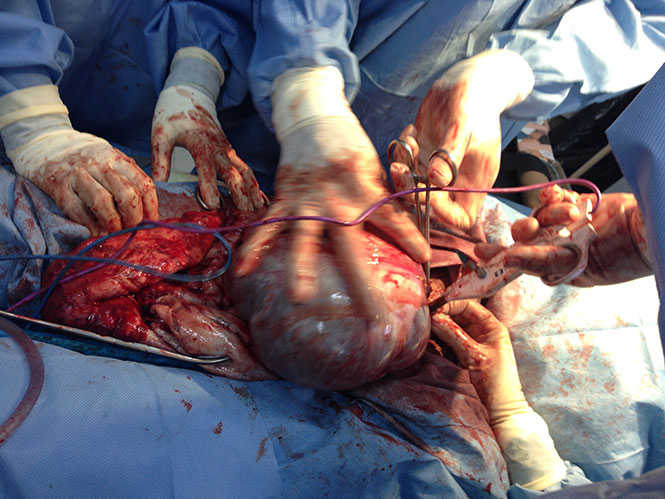
Giant Ovary


This patient is not pregnant. She had a giant ovarian tumor we removed by open surgery. Whereas, most surgeons would have cut her open with a 2-foot incision on her belly, we managed to remove this giant ovarian tumor with only a 6-inch incision, without spilling its contents inside the abdominal cavity!! Her abdomen went completely scaphoid after the giant space-occupying mass was removed l!!


Morcellated Myomata


To get a large specimen out of a 12 mm incision during a robotic surgery, we morcellate them in smaller chunks and extract then from the hole in the umbilicus!



