Monthly Archives: May 2018
WATERBIRTHING: A NEW YET ANCIENT PHILOSOPHY ON CHILDBIRITH

REBECCA B. SINGSON, MD, FPOGS, FPSCPC

Waterbirthing is a non-traditional concept of giving birth which consists of the baby being delivered under water, careful monitoring and management of the process of labor, and restrictive use of invasive methods. The mother’s wishes are prioritized, the natural process of birth is respected, medical intervention and techniques are minimized as long as the safety of the mother and child are not compromised. The mother usually enters the birthing pool or tub during labor with the water set at body temperature once she goes in to active labor. She may go in and out as she pleases depending on the pace of her labor. She may opt to give birth in the water of out of it. She and her partner decide the process of her birth in conjunction with their doctor or birth attendant.
WHAT ARE THE ADVANTAGES OF WATERBIRTHING FOR LABORING WOMEN?:
Waterbirthing can provide the hydrothermal effects of producing perineal and vaginal relaxation. It also provides hydrokinetic effects of releasing oxytocin from the mother’s brain due to nipple stimulation of water. It minimizes the need for medical intervention because when the woman is relaxed, she experiences less pain, thus leading to less anxiety, which in turn lowers adrenaline levels, encouraging the release of oxytocin and more oxygen flow to tissues.
Compared to a laboring woman lying in bed with the uterus compressing the inferior vena cava (the biggest vein returning blood flow to the heart), water birthing lowers compression of the big vessels. Thus, blood supply to the uterus and the placenta is improved. This results in the fetus benefiting with improved oxygenation. 1
WHAT ARE THE ADVANTAGES FOR BIRTHING WOMEN AND BABY?:
Waterbirthing provides a low-risk alternative to delivering on bed or in a stirrup. The element of water angles the process of birth so it is viewed as a wellness rather than an illness. The process restores the control of the birthing process to the mother. Since the water duplicates the amniotic fluid environment inside the uterus, waterbirthing provides a gentle transition to the world for the baby instead of a violent one. It is said to foster non-violence in the child when he becomes an adult.2
A prospective study of more nearly 6,000 mothers giving birth was performed at the clinic for obstetrics & gynecology of the cantonal hospital of Fauenfeld, Switzerland comparing over 2000 waterbirths to other methods of delivery like the Maia-birthing stool, birthing bed, Roma wheel, and others. It was noted that waterbirthing was the most popularly chosen alternative birth method adopted by 34-40% of mothers with spontaneous single births. It was found that the episiotomy rates were lowest after waterbirths and the 3rd and 4th degree lacerations occurred less frequently than bedbirths.
There is also significantly lower blood loss in waterbirths which could be due to the lower incidience of perineal lacerations and the hydrostatic pressure in t the tub preventing vessels from bleeding.
Women who delivered by waterbirthing needed less painkillers compared to any other birth method. This had to do with the relaxing effects of water and the facilitated movement in its weightlessness.
The results in the neonates’ birth parameters such as pH of the arterial umbilical cord blood and Apgar scores were better than other birth methods. In over 2000 waterbirths in the study, there was not a single case of aspiration, drowning or death as a result of waterbirthing.
WHAT ARE THE CONTRAINDICATIONS TO WATERBIRTHING?
Waterbirthing is contraindicated in the presence of any documented fetal distress. Maternal fever of greater than 100.4 of suspected maternal infection or amnionitis or a positive HIV status also contraindicate waterbirthing. Vaginal, urinary tract and skin infections, excessive vaginal bleeding, heavy meconium staining or any conditions requiring continuous electronic fetal monitoring are also contraindications. Prematurity of the fetus and malpresentation also contraindicates waterbirthing. 1
WON’T MY BABY ASPIRATE OR DROWN DURING WATERBIRTHING?
There is no valid report of a neonate that ever drowned or died after birth as a consequence of a waterbirth.3 This has been explained by the diving reflex – and inhibitory reflex associated with the larynx. The larynx has been found to have 5x more taste buds than the whole tongue surface. When any liquid reaches the back of the throat, the taste buds interpret what substance it is and the glottis closes automatically so the liquid is swallowed, not inhaled. This reflex, which is present in all babies till age six to eight months to facilitate breastfeeding, prevents water aspiration.4
So under normal circumstances, the baby won’t breathe or gasp under water. It is only if the fetus was experiencing severe and prolonged lack of oxygen or because on anesthesia, that it may then gasp as soon as it is born, possibly inhaling water into the lungs.5
The baby continues to breathe while underwater through the placenta until the baby is brought out of the water. It is only when the face comes in contact with air that the first breath will be taken. One possibility why a baby would lack oxygen under water, though, would be if the placenta detached prematurely as in the case of abruptio placenta.
WON’T THE MOTHER OR BABY GET INFECTED?
Some hospital restrict a woman with a ruptured waterbag to do waterbirthing. There is really no basis for that since the research shows that the water does not enter the vaginal canal. In 1960, Dr. Siegel reported in the American Journal of OBGyn that when he did experiments on 30 moms to place tampons in the vaginal then have the mom sit in a tub of iodinated water for 15 mins., not one tampon became stained in all cases. He, thus, concludes that women should not be restricted from bathing in the later stages of labor.6
Infections of the neonate were not more frequent with a waterbirth delivery than any other birth method in over 2000 babies studied.3 There are some studies, though that show otherwise. 7.8
Studies show that women who give birth in water have the most satisfying birth experience.3 Waterbirthing is more a philosophy on nonintervention than a method of giving birth. It embodies spiritual, psychological, technological, humanitarian and scientific aspects of birth that make a mother completely connected to her body. It requires a certain level of consciousness and responsibility to take over her birth process and work with her doctor to avoid untoward outcomes that will jeopardize her baby. Waterbirthing is as ancient as it is new. Water allows us to surrender to the greatest miracle that can happen to a woman. The miracle of childbirth.

- Rossi A, Cornette J, Johnson MR, et al. Quantitative cardiovascular magnetic resonance in pregnant women: cross-sectional analysis of physiological parameters throughout pregnancy and the impact of the supine position. J Cardiovasc Magn Reson. 2011;13:31.
- 2 http://www.gentlebirth.org/archives/watrbrth.html. Birth Without Violence. Frederick Leboyer
- Geissbuhler Verena, Eberhard Jakob, Waterbirths: A Comparative Study. Fetal Diagn Ther 2000:15:291-300.
- Harding, R., Johnson, P., McClelland, M. (1978) Liquid sensitive laryngeal receptors in the developing sheep, cat and monkey. J of Physiol 277:409-22.
- Fewell, J.E. Johnson, P., Mc Clelland, M. (1983). Upper airway dynamics during breathing and during apnea in fetal lambs. J of Physiol 339:495-504.
- Siegel, P. (1960), Does Bath water enter the vagina? Journal of Obstet & Gynecol 15:660-1.
- Rawal J. Shah A, Stirk F, Mehtar S: Waterbirth and infection in babies, BMJ 1994;209-511
- Hawkins S: Water vs. conventional births; Infection rates compared. Nurs Times 1995-91:38-40.
Labiaplasty
Labiaplasty is a plastic surgery procedure which involves altering the labia minora (inner labia) and the labia majora(outer labia), the folds of skin surrounding the vulva.
Labiaplasty has been practiced since the 1970’s when women thought that the labia minora should not protrude beyond the labia majora for aesthetic and fuctional satisfaction.1
Because there are not many images of the vulva on social media or even textbooks, women have limited access to knowledge on vulvar anatomy. Therefore, they are unable to say what a “normal” vulva looks like. Because pornographic images are so easily available on the internet, this is likely the probable source of comparison of women of their vulvar structures and it is not uncommon for a woman, dissatisfied with her anatomy to bring a photo from a porn site to demonstrate how they would like their genitals to look like.
In 2005, a study was reported on measurements of the average size, color and texture of the various parts of the female vulva and the following table was published at the British Journal of Obstetrics & Gynecology2:
Measurements |
Mean [standard deviation] | |
| Clitoral length (mm) | 5.0 – 35.0 | 19.1 [8.7] |
| Clitoral glans width (mm) | 3.0 – 10.0 | 5.5 [1.7] |
| Clitoris to urethra (mm) | 16.0 – 45.0 | 28.5 [7.1] |
| Labia majora length (cm) | 7.0 – 12.0 | 9.3 [1.3] |
| Labia minora length (mm) | 20 – 100 | 60.6 [17.2] |
| Labia minora width (mm) | 7.0 – 50.0 | 21.8 [9.4] |
| Perineum length (mm) | 15.0 – 55.0 | 31.3 [8.5] |
| Vaginal length (cm) | 6.5 – 12.5 | 9.6 [1.5] |
| Tanner Stage (n) | IV | 4.0 |
| Tanner Stage (n) | V | 46 |
| Color of the genital area
compared to the surrounding skin (n) |
Same color | 9.0 |
| Color of the genital area
compared to the surrounding skin (n) |
Darker color | 41 |
| Rugosity of the labia (n) | Smooth (unwrinkled) | 14 |
| Rugosity of the labia (n) | Moderately wrinkled | 34 |
| Rugosity of the labia (n) | Markedly wrinkled | 2.0 |
Despite this, there is still no current established aesthetic ideal as to how the labia minor should look like. However, it is a common consensus that labia minor protruding past the labia majora are both aesthetically and functionally considered unsatisfactory. Aside from the labia minora, the labia majora has also been perused especially when porn centerfold photography started to show the female genitalia more prominently than the female breast.
Because of the huge variations in the vulvar anatomy, a patient’s expectations have to be managed and tailored towards realistic expectations because just like with plastic surgery of the face, one cannot convert an Oprah Winfrey to an Angelina Jolie.
TECHNIQUES FOR LABIAPLASTY:
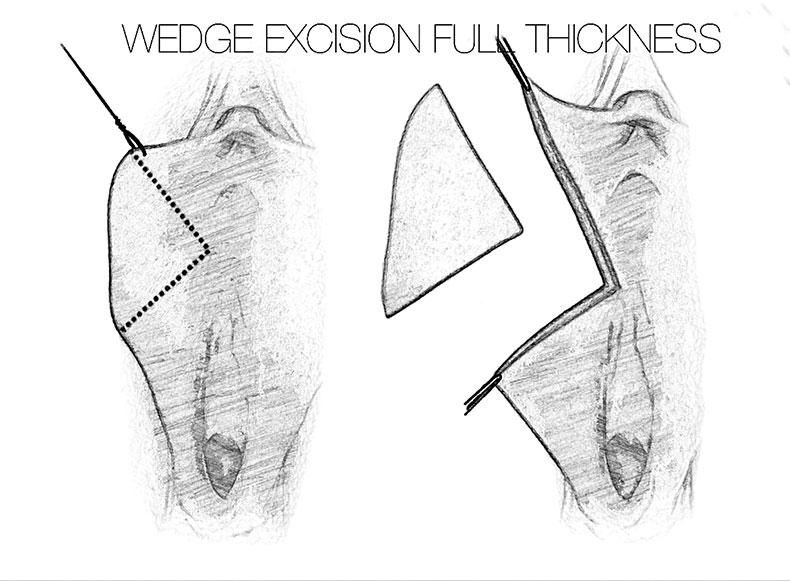
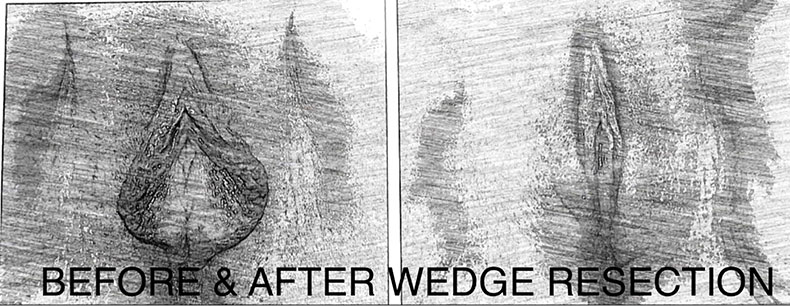
Wedge resection technique
It is rare for women who want labiaplasty to want to preserve the pigmented edge of their labia. For these cases, a wedge resection is ideal because central wedge-resection involves cutting and removing a partial-thickness wedge of tissue from the thickest portion of the labium minus. Unlike the edge-resection technique, the resection pattern of the central wedge technique preserves the natural rugosity (“wrinkled” edge) of the labia minora. If performed as a full-thickness resection, there is the risk of damaging some labial nerves, which can result in painful neuromas and numbness. A partial thickness removal of mucosa and skin, leaving the submucosa intact, decreases the risk of this complication.3 Furthermore, the central wedge-resection technique can be a tricky procedure since it is sometimes difficult to estimate the correct amount of labial skin to remove, so there is always the risk of either under-correction (persistent tissue-redundancy), or the overcorrection (excessive tension to the surgical wound),which may lead to increased probability either dissatisfaction or surgical wound dehiscence. One benefit, though is that extended wedge can be brought upwards towards the prepuce to treat a prominent clitoral hood without needing to create a separate incision.4 This leads to a natural contour for the finished result, and avoids direct incisions near the highly-sensitive clitoris.
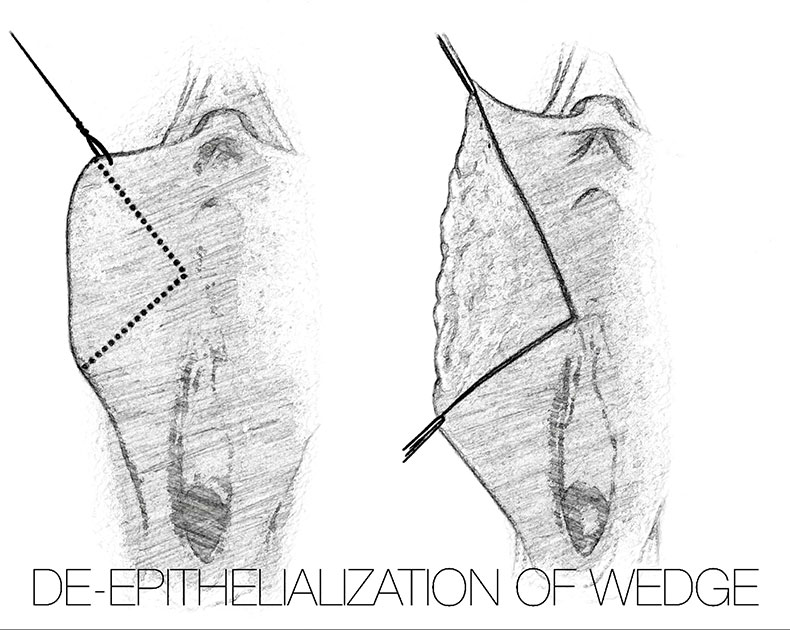
De-epithelialization/Demucosalization technique
For women with thin or atrophic labia, labial reduction by means of the de-epithelialization of the tissues is ideal. It involves cutting the epithelium of a central area on the inside and outside part of each labium minora, either with a scalpel or, low current pinpoint cautery, radiofrequency or laser knife. This method reduces the vertical excess tissue, while preserving the natural rugae (corrugated free-edge) of the labia minora. It plumps up the tissues since only the outer skin is removed plus it preserves the sensory and erectile characteristics of the labia. The disadvantage, though, of de-epithelialization is that the width of the individual labium might increase if a large area of labial tissue must be de-epithelialized to achieve the labial reduction.
Labiaplasty with Clitoral Unhooding
 Patients with large labia minora may also have a redundant or widened clitoral hood. This is where a labial reduction procedure may include the resection of the clitoral prepuce or clitoral hood when the thickness of its skin is considered unaesthetic to the patient or partner, or if it interferes with the woman’s sexual response. 5,6
Patients with large labia minora may also have a redundant or widened clitoral hood. This is where a labial reduction procedure may include the resection of the clitoral prepuce or clitoral hood when the thickness of its skin is considered unaesthetic to the patient or partner, or if it interferes with the woman’s sexual response. 5,6
Many waxing salons are sprouting in many countries, which Increases the awareness of women to wax their pubic hair. More women are choosing to use tight fitting gym outfits, swimwear and garments which can lead to more complaints of the labia minora getting caught mechanically or being abraded. It is also natural that women are getting more conscious of how their genitals appear.
Proper counseling needs to be given to women to assess the severity or deviation from normal anatomy, potential complications discussed before subjecting women to any procedure.
- Hamori CA. Aesthetic surgery of the female genitalia:labiaplasty and beyond. Plast Reconstr Surg 134:661, 2014.
- Lloyd, Jillian; Crouch, Naomi S.; Minto, Catherine L.; Liao, Lih-Mei; Creighton, Sarah M. (May 2005). “Female genital appearance: “normality” unfolds”. BJOG: An International Journal of Obstetrics & Gynaecology. Wiley. 112(5): 643–646.doi:10.1111/j.1471-0528.2004.00517.x. PMID15842291. Pdf.
- Alter, Gary J. (March 1998). “A new technique for aesthetic labia minora reduction”. Annals of Plastic Surgery. Wolters Kluwer. 40(3): 287–290.doi:10.1097/00000637-199803000-00016. PMID9523614.
- Alter, Gary J. (December 2008). “Aesthetic labia minora and clitoral hood reduction using extended central wedge resection”. Plastic and Reconstructive Surgery. Lippincott Williams & Wilkins. 122(6): 1780–1789.doi:10.1097/PRS.0b013e31818a9b25. PMID19050531.
- Hamori, Christine A. (1 September 2013). “Postoperative clitoral hood deformity after labiaplasty”. Aesthetic Surgery Journal. Oxford Journals. 33(7): 1030–1036.doi:10.1177/1090820X13502202. PMID24005612
- Hunter, John G. (1 September 2013). “Commentary on: postoperative clitoral hood deformity after labiaplasty”. Aesthetic Surgery Journal. Oxford Journals. 33(7): 1037–1038. doi:10.1177/1090820X13503476. PMID24081697.
10 SEXUAL TRUTHS YOU MUST KNOW

REBECCA B. SINGSON, MD, FPOGS, FACS, FPSCPC
- Men need to be wound up and excited during sex for them to achieve orgasm while women need to be relaxed with their partners to enjoy sex and reach peak pleasure.
- A man’s pleasure in sex is in the release of tension. He can go from foreplay to orgasm within 2 minutes. In contrast, a woman’s pleasure is in the gradual build-up of sexual tension and in fact, generally needs at least 20 mins. of foreplay before being ready for actual intercourse. She is like an oven than needs pre-heating. This is where a lot of men fall short. They think when they’re ready, their partner is ready. Unless the woman is dripping with lubrication, don’t attempt at intercourse because it’s a sign that her body in not ready. Doing so prematurely can lead to pain and laceration.
- There is an important purpose for this prolonged foreplay for women. There are 4 phases of the Human Sexual Response: the Excitement Phase, the Plateau Phase, the Orgasmic Phase and Resolution Phase. Excitement Phase is the phase of seduction which leads to the congestion of the organs. It takes around 20 mins. to get from Excitement Phase to Plateau Phase at which time the lower part of the vagina engorges to create friction (resulting in increased pleasure for the man), as well as for the vagina to lengthen. Vaginal lengthening is essential prior to intercourse because if the man starts thrusting before his partner’s vaginal canal has lengthened, he can induce a laceration at the end of the vagina and cause massive bleeding which has resulted at times in an emergency situation requiring suturing. (In my practice of 20 years, I have seen and managed 4 cases).
- Effective foreplay begins in the brain before you even touch each other’s bodies. Sexual turn ons for the woman: giving flowers, holding her hand, hugging her, complimenting her and her looks with big words like, “You are extremely irresistible”, “Your lips are so luscious”, “I’ve never met a sexier woman”. For the man, it’s rubbing his ego, allowing him his space, complimenting him on how good he is at turning you on. A sure turn off for a lot of men would be to choreograph his moves and be judgmental of him.
- Generally, a man’s satisfaction in sex relies in his ability to please his woman. A woman’s satisfaction in sex is in how well a man pleasures her. Or course, there are variants and extremes depending on how selfish or egoistic a person is.
- Orgasm for women is the release of sexual tension involving a response of all the muscles surrounding the vagina, anus and the uterus, contracting and repeating at 0.8 second intervals. The actual number and intensity of contractions varies from one woman to another but the important thing to remember is that the intensity of orgasm depends on the length of the Excitement Phase. That’s why it’s so important to spend a lot of time in foreplay because the longer and more excited you get your female partner to be, the more intense and pleasurable her orgasm will be.
- Orgasm is controlled by the sympathetic portion of the nervous system. This means that if you take some drugs like antihypertensives , or a big dose of alcohol which affect the sympathetic portion of the nervous system, it may interfere with your ability to achieve orgasm.
It had long been known that the center for orgasm of women was the clitoris until Grafenberg described the G-spot, which can be located this way: with the woman lying on her back, if her partner inserts a finger in the vagina with the palm facing the ceiling, on the anterior wall of the vagina within an inch from the opening, you can feel a 1×1 cm rough ridge, which when stimulated gives the woman the sensation she wants to pee. When stimulated rapidly alternating with or without clitoral stimulation, it can lead to an intense orgasm. - At the height of orgasm, some women release ejaculatory fluid from the urethra akin to the male prostatic fluid. It can be a generous amount and so may lead the woman and her partner to think she may have urinated. But in the absence of the smell of urine, this has got to be ejaculatory fluid.
- After an orgasm, women generally have no refractory period before reaching their next orgasm. Thus women can be multi-orgasmic. The men, in contrast, have a refractory period and need a period of time before achieving their next orgasm.
- Sexual satisfaction is one of the most important human experiences. However, as much as 50% of all married couples experience some sexual dissatisfaction, yet rate themselves to be happily married. This implies that sexual satisfaction not a necessary component to a happy marriage.
For women in menopause, hormone replacement therapy may greatly enhance a woman’s libido, promote vagina lubrication and prevent the vaginal atrophy that happens with the drop of estrogen. The thinning out of the vaginal walls results in dyspareunia or painful intercourse. This can be reversed with estrogen replacement which may be given Italy, transdermally or transvaginally.
Aside from hormones, vagina lasers administered intravaginally once a month for three months of the year can also promote vaginal lubrication and thickening, enhancing sexual satisfaction, removing the pain with intercourses, tightening the vagina after childbirth, and reversing mild to moderate incontinence (involuntary passing of urine when you cough or sneeze after childbirth.



